
What is Bell’s Palsy?
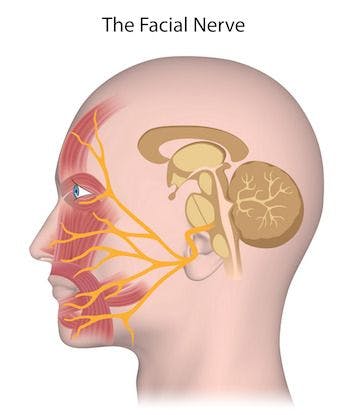
Bell’s palsy is a form of temporary facial paralysis resulting from damage or trauma to the facial nerves. The facial nerve-also called the 7th cranial nerve-travels through a narrow, bony canal (called the Fallopian canal) in the skull, beneath the ear, to the muscles on each side of the face. For most of its journey, the nerve is encased in this bony shell.
Each facial nerve directs the muscles on one side of the face, including those that control eye blinking and closing, and facial expressions such as smiling and frowning. Additionally, the facial nerve carries nerve impulses to the lacrimal or tear glands, the saliva glands, and the muscles of a small bone in the middle of the ear called the stapes. The facial nerve also transmits taste sensations from the tongue.
When Bell’s palsy occurs, the function of the facial nerve is disrupted, causing an interruption in the messages the brain sends to the facial muscles. This interruption results in facial weakness or paralysis.
Bell’s palsy is named for Sir Charles Bell, a 19th century Scottish surgeon who described the facial nerve and its connection to the condition. The disorder, which is not related to stroke, is the most common cause of facial paralysis. Generally, Bell’s palsy affects only one of the paired facial nerves and one side of the face, however, in rare cases, it can affect both sides.
How can Physical Therapy Help?
Physical therapy can help patients with Bell’s Palsy in the following ways:
- Facial massage to decrease pain.
- Facial exercise for subacute & chronic cases to improve facial nerve & muscle function.
- Education & instruction on eye protection (see below).
Eye Protection
Bell’s palsy can interrupt the eyelid’s natural blinking ability, leaving the eye exposed to irritation and drying. Therefore, keeping the eye moist and protecting the eye from debris and injury, especially at night, is important. Lubricating eye drops, such as artificial tears or eye ointments or gels, and eye patches are also effective.
In general, decompression surgery for Bell’s palsy — to relieve pressure on the nerve — is controversial and is seldom recommended. On rare occasions, cosmetic or reconstructive surgery may be needed to reduce deformities and correct some damage such as an eyelid that will not fully close or a crooked smile.
What are the symptoms?
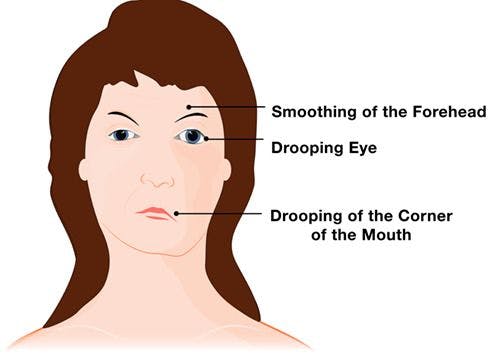
Because the facial nerve has so many functions and is so complex, damage to the nerve or a disruption in its function can lead to many problems. Symptoms of Bell’s palsy can vary from person to person and range in severity from mild weakness to total paralysis. These symptoms may include twitching, weakness, or paralysis on one or rarely both sides of the face. Other symptoms may include drooping of the eyelid and corner of the mouth, drooling, dryness of the eye or mouth, impairment of taste, and excessive tearing in one eye. Most often these symptoms, which usually begin suddenly and reach their peak within 48 hours, lead to significant facial distortion.
Other symptoms may include pain or discomfort around the jaw and behind the ear, ringing in one or both ears, headache, loss of taste, hypersensitivity to sound on the affected side, impaired speech, dizziness, and difficulty eating or drinking.
What causes Bell’s Palsy?
Bell’s palsy occurs when the nerve that controls the facial muscles is swollen, inflamed, or compressed, resulting in facial weakness or paralysis. Exactly what causes this damage, however, is unknown.
Most scientists believe that a viral infection such as viral meningitis or the common cold sore virus—herpes simplex—causes the disorder. They believe that the facial nerve swells and becomes inflamed in reaction to the infection, causing pressure within the Fallopian canal and leading to ischemia (the restriction of blood and oxygen to the nerve cells). In some mild cases (where recovery is rapid), there is damage only to the myelin sheath of the nerve. The myelin sheath is the fatty covering-which acts as an insulator-on nerve fibers in the brain.
The disorder has also been associated with influenza or a flu-like illness, headaches, chronic middle ear infection, high blood pressure, diabetes, sarcoidosis, tumors, Lyme disease, and trauma such as skull fracture or facial injury.
Who gets it?
Bell’s palsy afflicts approximately 40,000 Americans each year. It affects men and women equally and can occur at any age, but it is less common before age 15 or after age 60. It disproportionately attacks people who have diabetes or upper respiratory ailments such as the flu or a cold.
How is it diagnosed?
A diagnosis of Bell’s palsy is made based on clinical presentation — including a distorted facial appearance and the inability to move muscles on the affected side of the face — and by ruling out other possible causes of facial paralysis. There is no specific laboratory test to confirm diagnosis of the disorder.
Generally, a physician will examine the individual for upper and lower facial weakness. In most cases this weakness is limited to one side of the face or occasionally isolated to the forehead, eyelid, or mouth. A test called electromyography (EMG) can confirm the presence of nerve damage and determine the severity and the extent of nerve involvement. Blood tests can sometimes be helpful in diagnosing other concurrent problems such as diabetes and certain infections. A magnetic resonance imaging (MRI) or computed tomography (CT) scan can eliminate other structural causes of pressure on the facial nerve.
What is the prognosis?
The prognosis for individuals with Bell’s palsy is generally very good. The extent of nerve damage determines the extent of recovery. Improvement is gradual and recovery times vary. With or without treatment, most individuals begin to get better within 2 weeks after the initial onset of symptoms and most recover completely, returning to normal function within 3 to 6 months. For some, however, the symptoms may last longer. In a few cases, the symptoms may never completely disappear. In rare cases, the disorder may recur, either on the same or the opposite side of the face.